Faringo-Esophageal Diverticulum or Zenker's Diverticulum is a relatively rare disease of the esophagus that affects about 2 people per 100,000 inhabitants. It consists in the formation of an extroflexion (a sort of bag) in the initial part of the esophagus, exactly at the point of passage from the pharynx to the esophagus.
5 POST-OPERATIVE INFORMATION
Zenker's diverticulum is formed in a particularly weak area of the pharynx-esophageal tract in which the transverse muscle fibers of the pharynx (Cricopharyngeal muscle) and the oblique fibers of the inferior constrictor muscle form a triangle called the Killian triangle. When, due to a defect in the motility of the esophagus and in particular the upper esophageal sphincter muscle, the bolus (that is, the chewed and ingested food) finds it difficult to enter the esophagus, generates an outward pressure through the weak point (Killian's triangle) forming the bag, the diverticulum called Diverticulum by Zenker (from the name of Dr. Zenker who together with Von Ziemssen in 1877 reviewed all the data published in the world on patients with pharynx-esophageal diverticula). Most striking adult males often over 75 years of age in a ratio of 1 to 5 compared to the female gender.
SYMPTOMS:
The most frequent symptom is the difficulty in swallowing (DYSFAGIA), often associated with PAIN and SWELLING in the neck, generally in the left side. The stagnation of food in the diverticulum can last a long time and patients report REGURGITATION of food ingested even after several days, obviously associated with FOUL BREATH. Regurgitation can sometimes lead to inhalation of food in the respiratory tree resulting in PULMONARY INFECTIONS up to severe ASPIRATION PNEUMONIA.
DIAGNOSIS:
Although the diagnosis is often made during an ESOPHAGOGASTROSCOPY, the best examination is an X-ray during barium ingestion, a so-called BARIUM SWALLOWING EXAMINATION. In fact, endoscopic examination must be performed by expert personnel, very cautiously, as if the endoscope enters the diverticulum it could tear it. Generally for completeness of study I also perform a CT scan of the neck and thorax to rule out pulmonary complications. I do not considerthe necessity an Esophageal Manometry (the study of the pressure of the esophagus during swallowing) because it often gives inconclusive results (it is believed that the presence of the diverticulum per se does not allow an optimal manometric study), besides being a troublesome exam for the patient .
TREATMENT:
There are two possibilities of treatment of the Diverticulum Faringo - Esophageal of Zenker, one SURGICAL through an incision of the neck and one ENDOSCOPIC.
SURGICAL TREATMENT .
There are two main surgical procedures for the treatment of Zenker's diverticula: diverticulectomy with myotomy and & nbsp; Diverticolopexia with myotomy.
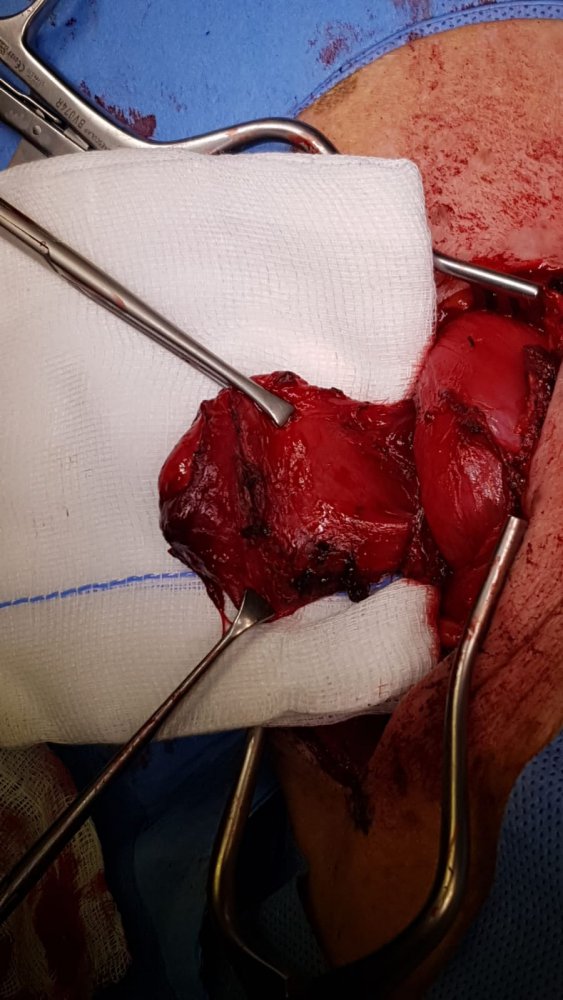
1) DIVERTICOLECTOMY with MIOTOMIA.
It's the treatment I've been doing for many years. It consists in making an incision in the left neck, isolating the diverticulum, dissecting it (diverticulectomy) with a stapler that dissects and simultaneously sews the base of the diverticulum.
Then the muscle fibers of the esophagus below the diverticulum (myotomy) are dissected to release the esophagus and prevent recurrence of the diverticulum.
It is a delicate operation that is relatively low traumatic and should be performed only by experienced surgeons since one operates very close to vascular and nerve structures which must be absolutely respected, such as the carotid artery, the jugular vein, the vagus nerve, the phrenic nerve, the laryngeal nerve (which provides the innervation of the vocal cord).
The more fearsome complication although rare is the possibilty of the dehiscence of the esophageal suture; resulting in neck infection and sometimes need of a reoperation.
2) DIVERTICOLOPESSIA con MIOTOMIA.
It differs from the previous intervention in that the diverticulum is isolated but instead of sectioning it is turned upwards and is fixed in this position so that the food cannot accumulate due to gravity. The second part, the myotomy, is also performed.
Although less decisive, it has the advantage of not affecting the diverticulum avoiding the possible dehiscence of the suture.
ENDOSCOPIC TREATMENT
It is a less invasive, transoral treatment, ie. through the mouth which provides a section of the septum between the diverticulum and the esophagus or the opening of the entire wall of the diverticulum in the esophagus. The latter procedure is identified by the acronym ESET (Endoscopic Stapler Esophagus- Diverticolotomy) ; Although not easy to understand I will try to explain the mechanism. A Stapler is inserted into the esophagus, ie. a stapler with two branches. One branch enters the diverticulum and the other enters the adjacent esophagus. When the two branches are closed (imagine the two parts of a stapler), these join the diverticulum wall to the esophagus. At this point the stapler cuts and sews these two walls at the same time. The final result is not the elimination of the diverticulum, but the annexation of the diverticulum to the esophagus which at that point will appear dilated but will not have that cavity constituted by the diverticulum and will not be able to stagnate the food waste.
Even in this case, the complications are represented by the possible lesion of the contiguous nerves or by the Deiscenza, ie from the lack of scarring between the diverticulum and the esophagus resulting in infection and mediastinitis.
This procedure is very difficult and needs adequate preparation and training. Therefore due to the low frequency of this pathology, there are not many endoscopists or centers that practice it.




{kind=link}
{kind=link}
{kind=link}