Achalasia consists in the lack of release of the esophagus's distal part at the passage of ingested food. Virtually when the food runs along the esophagus, it stops immediately above the stomach because the lower esophageal sphincter (LES) does not open up a sort of valve present between the esophagus and the stomach.
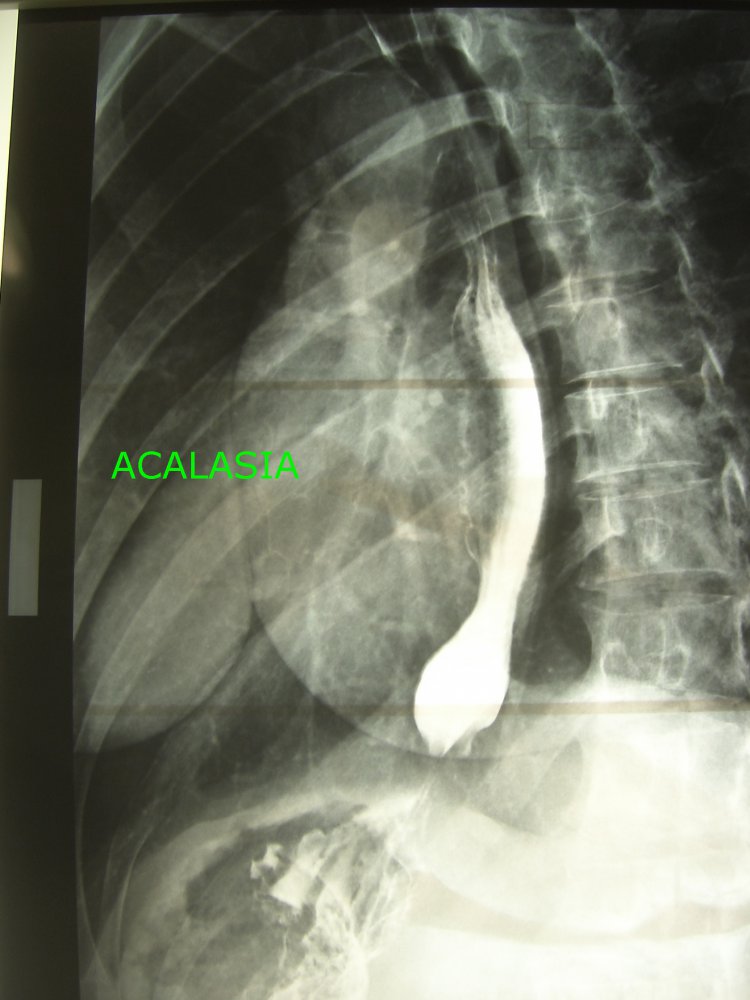
Acalasia , togheter with the Esophageal DIverticula, is one of the most important causes of bad swallowing (dysphagia), difficulty in passing food along the esophagus, swelling during swallowing (Odinophagia), regurgitation of un-digested food often associated with alitoid and weight loss. It does not know the cause except in some South American countries where it is caused by a parasitic infection and is called: Chagas Disease. With the progression of the disease, the esophagus that is a uniform tube dilates and extends abnormally. (Dolico-megaesophagus). See the photo. Symptoms are those described, and dysphagia, that is, the difficulty of swallowing is often called "paradoxical dysphagia" because the patient is able to swallow the solid foods of the liquid ones better. The diagnosis of acalasia is based on the EsophagusGastroDuodenoscopy (EGDS), the Esophagogram with Barito meal (contrast medium), and some more complex examinations such as Impedienceometry or Esophageal Manometry that allows to study the motility of the esophagus , THERAPY: Therapy aims to reduce the tone of the last stretch of the esophagus (LES) to allow easy food passage into the stomach. After an attempt to medical therapy and if the general conditions allow it you can try one: 1) Pneumatic dilation with balloon. Through the endoscopy, an inflatable balloon is placed in the diseased area of the esophagus and "splinks" the bowel musculature. The procedure is effective in 70% of patients, but it has a risk of about 3% to cause a perforation of the esophagus. 2) Botulinum toxin injection. Botulinum toxin is used for many purposes for its ability to paralyze muscle fibers at the injection site. Therefore also in Acacia is used to release the muscular fibers of the distal esophagus. It has very few contraindications but the effect lasts up to an average of 6 months. 3) Esophagomyotomy. The surgical procedure is called MIOTOMIA SECOND HELLER and consists of a delicate and selective section of the muscular fibers of the final part of the esophagus. Success is immediate and solves the problem in 95% of cases. As a result of the release, gastroesophageal reflux develops. That is why Miotonia is associated with anti-inflammatory plastic. As with other interventions, there are two SURGICAL TECHNIQUES: a Laparotomy, performed routinely up to about 10 years ago, and a Laparoscopic which represents the technique I used: MIOTOMIA LAPAROSCOPIC with SECOND DOR. It is performed with a few mm mini in the abdomen, the final part of the esophagus is prepared and with extreme precision, the muscular fibers that go outside the bowels are cut off as if to cover it. At the end, a stretch of stomach is wound around the esophagus to construct a new valve that prevents reflux of acid juice between the stomach and the esophagus. However, the patient will be advised to use drugs that prevent the production of acid juice. For the sake of information I would like to add that there is a new endoscopic technique called P.O.E.M. (For Oral Endoscopic Miotomy). During Endoscopy, a miniincision of the upper esophagus is performed in the area to be treated and a tunnel is created between the mucous membrane and the musculature of the esophagus until it reaches the area to be treated where the fibers involved are affected. The engraved mucosa is sutured with clips. There is also the possibility of Esophageal perforation and we have to wait for the results of clinical studies indicating the superiority of this method compared to the traditional one



{kind=link}
{kind=link}